Intravitreal injections (CPT 67028) are among the highest-volume and highest-revenue procedures in ophthalmology. Yet, they are also one of the most denial-prone services—especially when drug billing, modifiers, and documentation don’t align perfectly.
At Solubillix, we’ve audited thousands of retina and ophthalmology claims. The pattern is clear: most denials are preventable.
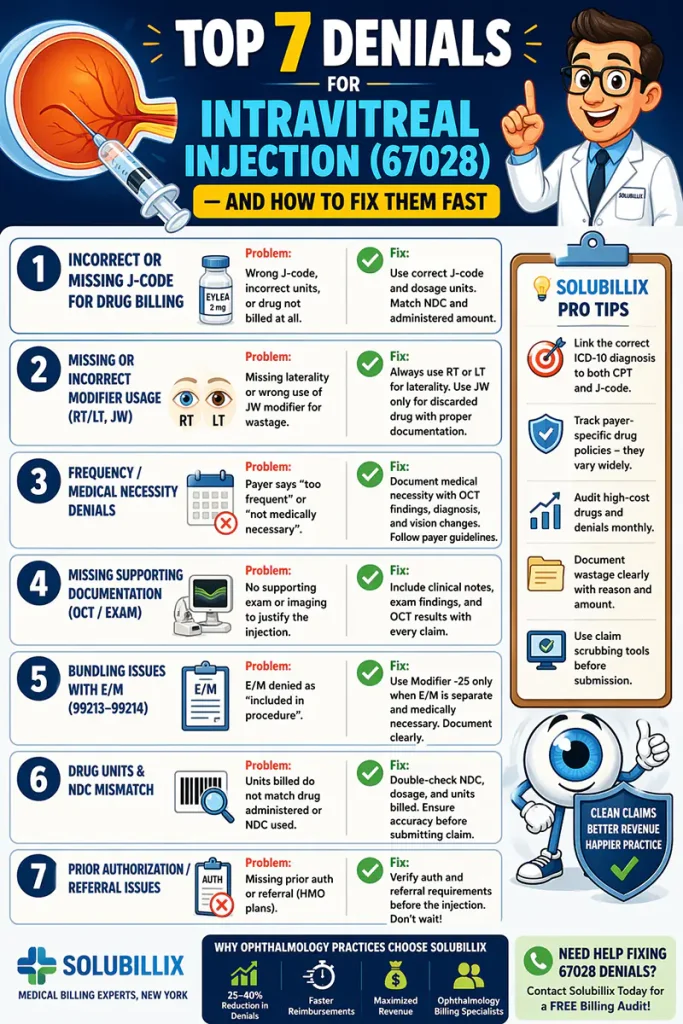
Here are the Top 7 denials for 67028—and exactly how to fix them fast.
🔴 1. Incorrect or Missing J-Code for Drug Billing
❌ The Problem:
Intravitreal injections require separate billing for the drug, but:
- Wrong J-code used
- Units don’t match dosage
- Drug not billed at all
💊 Common drugs:
- Aflibercept
- Ranibizumab
- Faricimab
- Bevacizumab
✅ The Fix:
- Verify correct J-code + dosage units
- Match units to NDC + administered amount
- Ensure drug and 67028 are billed together
🔴 2. Missing or Incorrect Modifier Usage (RT/LT, JW)
❌ The Problem:
- Missing RT/LT (laterality)
- Incorrect use of JW modifier for wastage
- Billing both eyes incorrectly
✅ The Fix:
- Always append:
- RT (right eye) or LT (left eye)
- Use JW only for discarded drug
- Document wastage clearly in note
👉 Tip: Many payers auto-deny claims without laterality.
🔴 3. Frequency / Medical Necessity Denials
❌ The Problem:
Payers flag:
- “Too frequent injections”
- “Not medically necessary”
Common diagnoses:
- Wet AMD
- Diabetic macular edema
- Retinal vein occlusion
✅ The Fix:
- Document:
- Disease progression
- OCT findings
- Vision changes
- Follow payer-specific frequency guidelines
👉 No documentation = automatic denial.
🔴 4. Missing Supporting Documentation (OCT / Exam)
❌ The Problem:
Billing 67028 without:
- Supporting exam
- Imaging like OCT (CPT 92134)
✅ The Fix:
- Ensure chart includes:
- Clinical indication
- Imaging results
- Provider assessment
👉 Strong documentation = faster approvals
🔴 5. Bundling Issues with E/M (99213–99214)
❌ The Problem:
E/M gets denied as:
- “Included in procedure”
- “Not separately identifiable”
✅ The Fix:
- Use Modifier -25 on E/M only if justified
- Document:
- Separate evaluation
- Decision-making beyond injection
👉 Not every visit qualifies for E/M billing
🔴 6. Drug Units & NDC Mismatch
❌ The Problem:
- Units billed ≠ drug administered
- NDC not aligned with claim
✅ The Fix:
- Cross-check:
- NDC number
- Dosage administered
- Units billed
👉 This is a top audit trigger in 2026
🔴 7. Prior Authorization / Referral Issues
❌ The Problem:
- Missing prior auth (common with commercial plans)
- Referral required but not obtained
✅ The Fix:
- Verify:
- Auth requirements BEFORE injection
- Referral (HMO plans)
👉 Retro auth rarely works—prevent upfront
💡 Pro Tips from Solubillix (What Most Practices Miss)
✔ Always link correct ICD-10 diagnosis to both CPT and J-code
✔ Track payer-specific drug policies (they vary widely)
✔ Audit high-cost drugs monthly
✔ Watch for wastage documentation gaps
✔ Use claim scrubbing tools before submission
🚀 Why Ophthalmology Practices Choose Solubillix
At Solubillix, we specialize in:
- Retina & ophthalmology billing
- High-value injection optimization
- Denial management & AR recovery
📈 Our clients typically see:
- 25–40% reduction in denials
- Faster reimbursements
- Improved revenue per injection
📞 Need Help Fixing 67028 Denials?
If your practice is struggling with:
- Injection denials
- Underpaid drug claims
- Complex payer rules
👉 Solubillix can help.
Contact us today for a free billing audit.
By Solubillix – Medical Billing Experts, New York