For family medicine practices, OB/GYNs, and community health centers, intrauterine device (IUD) placement is a fundamental component of comprehensive women’s health services. Yet, while the clinical side of the procedure is routine, the financial administration behind it is notoriously complex.
Every year, independent practices lose thousands of dollars in revenue due to simple administrative oversight: mismatched NDC numbers, improperly applied modifiers, omitted supply codes, and poorly documented medical necessity.
At Solubillix, we specialize in eliminating these administrative burdens. We provide 99% accurate medical billing and coding services designed to streamline workflows, slash denial rates, and maximize practice revenue. To protect your bottom line, we have constructed this definitive master guide to navigating CPT Code 58300 and its associated billing requirements.
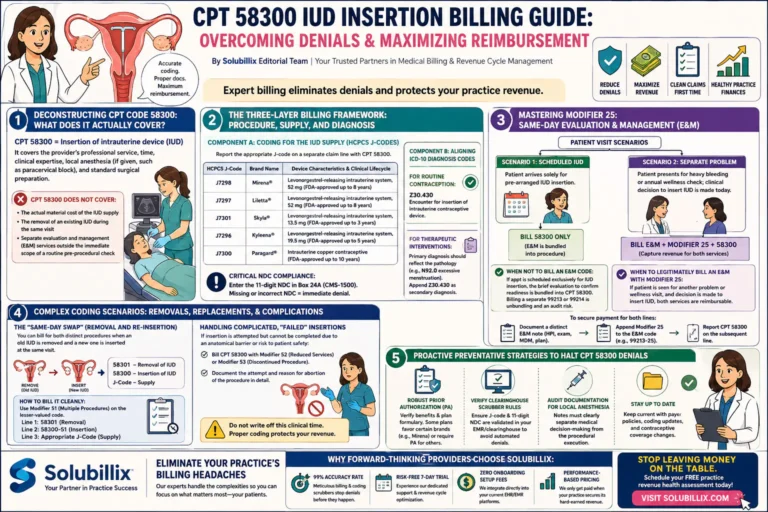
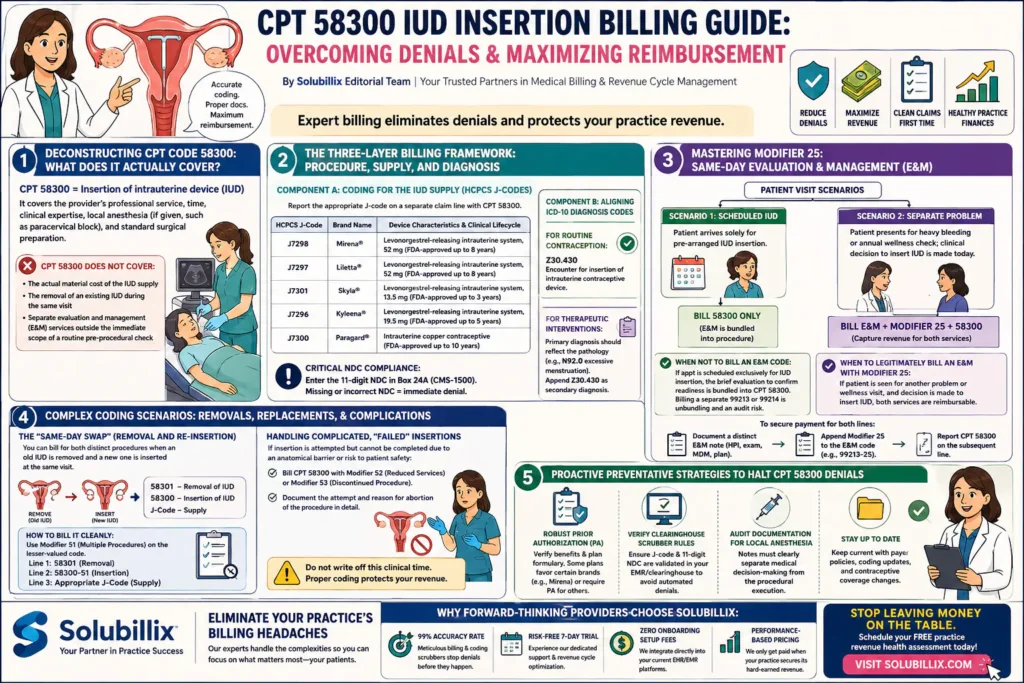
1. Deconstructing CPT Code 58300: What Does It Actually Cover?
According to the American Medical Association (AMA), CPT code 58300 is defined as: Insertion of intrauterine device (IUD).
It is critical to recognize that CPT 58300 represents the professional service of performing the procedure itself. It accounts for the provider’s time, clinical expertise, local anesthesia (if administered, such as a paracervical block), and standard surgical preparation.
Crucially, CPT 58300 does not cover:
- The actual material cost of the IUD supply.
- The removal of an existing IUD during the same visit.
- Separate evaluation and management (E&M) services that fall outside the immediate scope of a routine pre-procedural check.
Without an advanced billing infrastructure, practices often leave revenue on the table by assuming the single procedure code encapsulates the entire encounter.
2. The Three-Layer Billing Framework: Procedure, Supply, and Diagnosis
To build an unassailable insurance claim that passes through clearinghouses cleanly on the first submission, your practice must implement a structured, three-layer billing approach. Mismatches between these layers are a leading cause of claim rejections.
Component A: Coding for the IUD Supply (HCPCS J-Codes)
Unless your patient is acquiring their device via a specialty pharmacy that bills the carrier directly, your practice must absorb the upfront cost of the device inventory. To get reimbursed for that capital outlay, you must attach the appropriate HCPCS J-code on a separate claim line alongside CPT 58300.
| HCPCS J-Code | Brand Name | Device Characteristics & Clinical Lifecycle |
| J7298 | Mirena® | Levonorgestrel-releasing intrauterine system, 52 mg (FDA-approved up to 8 years) |
| J7297 | Liletta® | Levonorgestrel-releasing intrauterine system, 52 mg (FDA-approved up to 8 years) |
| J7301 | Skyla® | Levonorgestrel-releasing intrauterine system, 13.5 mg (FDA-approved up to 3 years) |
| J7296 | Kyleena® | Levonorgestrel-releasing intrauterine system, 19.5 mg (FDA-approved up to 5 years) |
| J7300 | Paragard® | Intrauterine copper contraceptive (FDA-approved up to 10 years) |
Critical NDC Compliance Note: Most commercial insurance payers and managed care Medicaid plans require the 11-digit National Drug Code (NDC) to be explicitly printed in Box 24A of the CMS-1500 form (or the electronic loop equivalent). A missing, outdated, or improperly formatted NDC number will cause an immediate, automated line-item denial for the expensive supply code.
Component B: Aligning ICD-10 Diagnosis Codes
Medical necessity is the benchmark of modern claims processing. Your diagnosis coding must perfectly align with the provider’s clinical intent.
- For Routine Contraception: The primary diagnosis code must be Z30.430 (Encounter for insertion of intrauterine contraceptive device).
- For Therapeutic Interventions: If a hormone-releasing LNg-IUD (like Mirena) is being placed primarily to treat secondary conditions such as menorrhagia (heavy menstrual bleeding) or dysmenorrhea, the primary ICD-10 code should reflect the pathology (e.g., N92.0 for excessive or frequent menstruation), while Z30.430 can be appended as a secondary diagnosis code.
3. Mastering Modifier 25: Same-Day Evaluation & Management (E&M)
The misuse—or complete omission—of Modifier 25 (Significant, separately identifiable evaluation and management service by the same physician on the same day of the procedure or other service) is arguably the greatest source of lost revenue in reproductive health billing.
[ PATIENT VISIT SCENARIOS ]
|
———————————————–
| |
[ SCENARIO 1: Scheduled IUD ] [ SCENARIO 2: Separate Problem ]
Patient arrives solely for Patient presents for heavy bleeding
pre-arranged IUD insertion. or annual wellness check; clinical
decision to insert IUD is made today.
| |
[ BILL 58300 ONLY ] [ BILL E&M + MODIFIER 25 + 58300 ]
(E&M is bundled into procedure) (Capture revenue for both services)
When NOT to Bill an E&M Code:
If a patient has an appointment scheduled exclusively for an IUD insertion, the brief evaluation required to confirm her readiness (such as checking vitals, performing a baseline pelvic assessment, and obtaining informed consent) is considered bundled into CPT 58300. Billing a separate 99213 or 99214 in this scenario constitutes unbundling and poses a significant audit risk.
When to Legitimately Bill an E&M with Modifier 25:
If a patient schedules an appointment to discuss a specific problem (e.g., pelvic pain, contraceptive counseling, or irregular bleeding), or presents for a routine preventive check-up, and during that encounter the clinical decision is made to proceed with an immediate IUD insertion, both services are separately reimbursable.
To secure payment for both lines, your billers must:
- Document a separate, stand-alone E&M note detailing the history, physical exam, and decision-making process that led to the procedure.
- Append Modifier 25 to the E&M code (e.g., 99213-25).
- Report CPT 58300 on the subsequent line.
4. Complex Coding Scenarios: Removals, Replacements, and Complications
Clinical realties are rarely perfectly linear. Providers routinely navigate nuanced cases that require expert coding adaptations to preserve revenue.
The “Same-Day Swap” (Removal and Re-insertion)
When a patient presents to have an expired or expiring IUD removed and a brand-new device inserted during the exact same clinical session, you are legally entitled to bill for both distinct procedures.
- CPT 58301 – Removal of intrauterine device (IUD)
- CPT 58300 – Insertion of intrauterine device (IUD)
How to bill it cleanly: Most major insurance clearinghouses and payers require Modifier 51 (Multiple Procedures) attached to the lesser-valued code to indicate that multiple distinct interventions occurred. Depending on regional payer rules, the claim should typically look like this:
- Line 1: 58301 (Removal)
- Line 2: 58300-51 (Insertion)
- Line 3: Appropriate J-Code (Supply)
Handling Complicated, “Failed” Insertions
What happens if a provider attempts to insert an IUD, encounters an anatomical barrier (such as severe cervical stenosis), cannot pass the internal os, and is forced to abort the procedure for patient safety?
Do not write off this clinical time. If the provider performed the work but could not successfully complete the placement, bill CPT 58300 with Modifier 52 (Reduced Services) or Modifier 53 (Discontinued Procedure), depending on whether the procedure was halted due to technical limitations or risk to patient well-being. Detailed operative notes detailing the attempt must accompany the claim during the appeals or review process.
5. Proactive Preventative Strategies to Halt CPT 58300 Denials
Even though the Affordable Care Act (ACA) mandates that most commercial health plans cover women’s preventive services—including contraception—without patient cost-sharing, payers aggressively find technicalities to delay or deny claims. Here is how your administrative team can stay ahead:
- Robust Prior Authorization (PA): While contraceptive procedures are generally covered, specific plan formularies may favor certain brands over others (e.g., approving Mirena but requiring a PA for Liletta). Always complete a comprehensive verification of benefits prior to the patient arriving in the exam room.
- Verify Clearinghouse Scrubber Rules: Ensure your electronic medical record (EMR) and clearinghouse software have built-in validation rules that cross-reference the J-code with the 11-digit NDC format.
- Audit Documentation for Local Anesthesia: Payers occasionally deny Modifier 25 claims if they believe the office visit was merely an excuse to administer a paracervical block. Your provider notes must clearly differentiate the medical decision-making from the procedural execution.
Eliminate Your Practice’s Billing Headaches with Solubillix
Managing the intricacies of family medicine and women’s health billing can exhaust an independent clinic’s internal staff. Hours spent chasing down denied J-codes or appealing bundled E&M lines are hours diverted from patient care.
At Solubillix, we act as a seamless extension of your healthcare practice. Operating across New York and nationwide, our billing specialists possess deep expertise in top industry software—including eClinicalWorks, Tebra (Kareo), NextGen, PracticeFusion, Athenahealth, and OfficeAlly.
Why Forward-Thinking Providers Choose Solubillix:
- 99% Accuracy Rate: Our meticulous billing and coding scrubbers stop denials before they happen.
- Risk-Free 7-Day Trial: Experience our dedicated support and revenue cycle optimization before committing.
- Zero Onboarding Setup Fees: We integrate directly into your current EHR/EMR platforms with absolute transparency.
- Performance-Based Pricing: We only get paid when your practice secures its hard-earned revenue.
Stop allowing insurance companies to withhold your legitimate reimbursements. Partner with the industry experts who know how to unlock every dollar on your fee schedule.
Ready to maximize your clinic’s financial performance? Visit Solubillix today to schedule your comprehensive, free practice revenue health assessment.