Dermatology practices perform thousands of lesion destruction procedures every year. While CPT 17000 and CPT 17003 appear straightforward, they remain among the most frequently underpaid, denied, and audited dermatology procedure codes due to documentation deficiencies, incorrect lesion counts, modifier errors, and payer-specific billing requirements.
At Solubillix, our dermatology billing specialists help providers optimize reimbursement, reduce denials, and maintain coding compliance across commercial insurance, Medicare, and Medicaid plans. This comprehensive guide explains how to correctly bill CPT 17000 and 17003 while avoiding common revenue cycle mistakes.
Understanding CPT 17000 and CPT 17003
Premalignant lesions, such as actinic keratoses (AKs), are commonly treated through cryosurgery, electrosurgery, laser destruction, chemosurgery, or surgical curettement.
CPT 17000
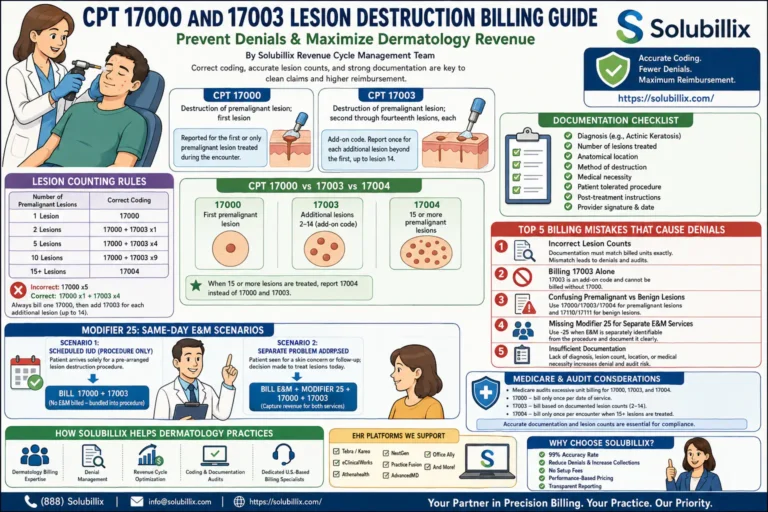
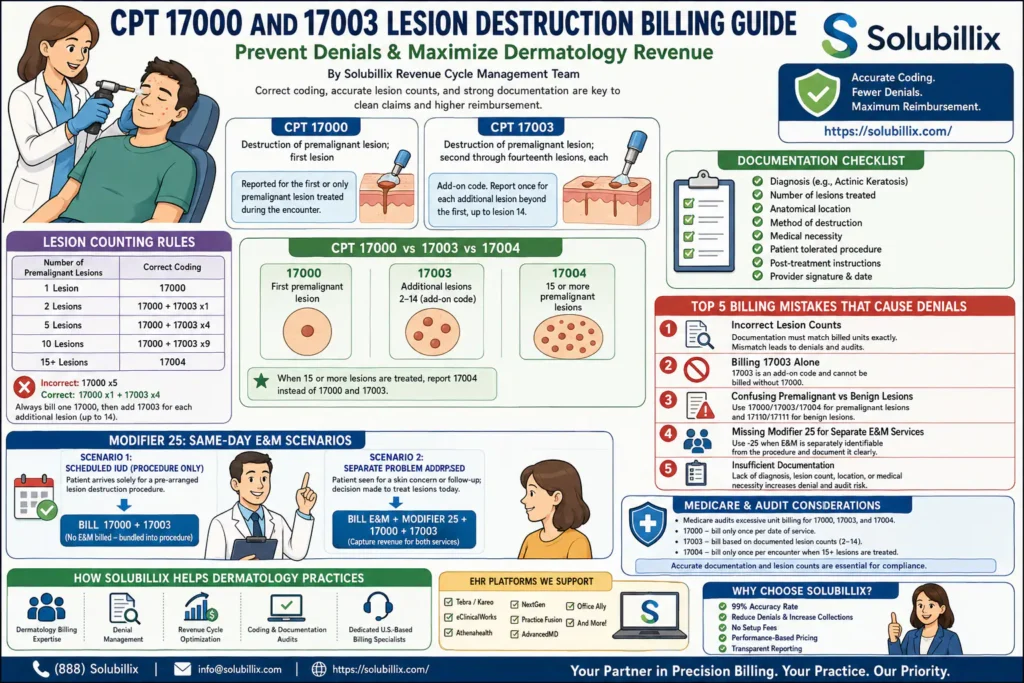
Destruction of premalignant lesion; first lesion
This code is reported for the first or only premalignant lesion treated during the encounter.
CPT 17003
Destruction of premalignant lesion; second through fourteenth lesions, each
This is an add-on code and must always be billed alongside CPT 17000. It is reported once for each additional lesion beyond the first, up to lesion number fourteen.
Lesion Counting Rules Every Dermatology Practice Must Know
One of the biggest causes of lost revenue is incorrect lesion counting.
| Number of Premalignant Lesions | Correct Coding |
| 1 Lesion | 17000 |
| 2 Lesions | 17000 + 17003 x1 |
| 5 Lesions | 17000 + 17003 x4 |
| 10 Lesions | 17000 + 17003 x9 |
| 15+ Lesions | 17004 |
Many practices mistakenly bill:
❌ 17000 x5
Instead of:
✅ 17000 x1 + 17003 x4
This error frequently leads to claim denials and underpayment.
CPT 17000 vs CPT 17003 vs CPT 17004
Understanding when to transition to CPT 17004 is critical.
| CPT Code | Description |
| 17000 | First premalignant lesion |
| 17003 | Additional lesions 2-14 (add-on code) |
| 17004 | 15 or more premalignant lesions |
Once the provider treats 15 or more premalignant lesions, CPT 17004 replaces both 17000 and 17003. Do not bill all three together.
Top 5 Billing Mistakes That Cause CPT 17000 and 17003 Denials
1. Incorrect Lesion Counts
Insurance auditors routinely compare procedure notes against billed units.
If documentation states:
“Cryotherapy applied to eight actinic keratoses”
The claim should reflect:
- 17000 × 1
- 17003 × 7
Failure to match lesion counts may trigger denials or post-payment audits.
2. Billing CPT 17003 Alone
CPT 17003 is an add-on code.
It cannot be submitted by itself.
Correct:
✅ 17000 + 17003
Incorrect:
❌ 17003 only
Most clearinghouses automatically reject standalone 17003 claims.
3. Confusing Premalignant and Benign Lesions
A common coding error occurs when providers confuse:
Premalignant Lesions
- Actinic keratosis
- Solar keratosis
Use:
- 17000
- 17003
- 17004
Benign Lesions
- Seborrheic keratosis
- Common warts
- Plantar warts
Use:
- 17110
- 17111
Selecting the wrong code family is a frequent reason for payer denials.
4. Missing Modifier 25 for Separate E&M Services
Many dermatology visits involve evaluation and treatment on the same day.
Appropriate Example
Patient presents for:
- New suspicious skin lesions
- Comprehensive skin examination
- Medical decision-making
- Cryotherapy treatment
Billing may include:
- 99213-25
- 17000
- 17003
The provider must clearly document a separately identifiable E&M service beyond the procedure itself.
Without sufficient documentation, payers often deny the office visit.
5. Insufficient Documentation
Insurance carriers increasingly request medical records for lesion destruction procedures.
Documentation should include:
✓ Diagnosis
✓ Lesion count
✓ Anatomical location
✓ Destruction method
✓ Medical necessity
✓ Provider signature
✓ Date of service
Incomplete documentation significantly increases audit risk.
Documentation Checklist for Audit-Proof Claims
At Solubillix, our dermatology billing specialists recommend documenting:
Lesion Details
- Number of lesions treated
- Exact anatomical locations
- Clinical diagnosis
Procedure Details
- Cryotherapy
- Electrosurgery
- Laser destruction
- Curettage
Treatment Response
- Patient tolerated procedure
- Post-treatment instructions provided
Medical Necessity
Clearly explain why lesion destruction was medically necessary.
The more specific the note, the easier it becomes to defend reimbursement during payer audits.
Medicare and Audit Considerations
Medicare has identified excessive unit billing for CPT 17000, 17003, and 17004 as an audit target.
According to CMS guidance:
- CPT 17000 should only be billed once per date of service.
- CPT 17003 should only be billed according to documented lesion counts.
- CPT 17004 should only be reported once per encounter when 15 or more lesions are treated.
This makes accurate documentation and lesion counting essential for compliance.
How Solubillix Helps Dermatology Practices Maximize Revenue
At Solubillix Medical Billing Services, we help dermatologists, Mohs surgeons, family medicine providers, and skin cancer clinics optimize reimbursement through:
Dermatology-Specific Billing Expertise
- CPT 17000–17004 billing
- Biopsy coding
- Mohs surgery billing
- Skin excision coding
- Pathology billing integration
Denial Management
- Modifier review
- Documentation audits
- Appeal preparation
- LCD and payer compliance verification
Revenue Cycle Optimization
- Charge capture review
- Coding audits
- AR follow-up
- Insurance verification
- Payment posting
EHR Platforms We Support
- Tebra/Kareo
- eClinicalWorks
- Athenahealth
- NextGen
- Practice Fusion
- AdvancedMD
- Office Ally
Final Thoughts
Although CPT 17000 and CPT 17003 appear simple, incorrect lesion counting, documentation gaps, and coding errors can quickly turn routine dermatology procedures into major revenue leaks.
By implementing proper coding workflows and maintaining detailed clinical documentation, providers can significantly reduce denials while maximizing reimbursement.
If your dermatology practice struggles with lesion destruction claim denials, modifier issues, or revenue cycle inefficiencies, Solubillix can help streamline your billing operations and improve collections.
Ready to improve your dermatology revenue cycle?
Visit Solubillix.com and schedule a free billing assessment today.