Retinal imaging plays a critical role in modern ophthalmology and optometry practices. However, many providers unknowingly lose revenue because of incorrect billing between CPT 92250 and CPT 92134. Although both codes involve retinal imaging, they represent entirely different diagnostic services with separate documentation requirements, reimbursement rules, and payer expectations.
At Solubillix, we frequently identify billing errors where ophthalmology practices use the wrong retinal imaging code, leading to denied claims, underpayments, compliance risks, and audit exposure. Understanding the distinction between these two CPT codes is essential for maintaining clean claims and protecting practice revenue.
Accurate coding is not only important for reimbursement—it is also critical for regulatory compliance and long-term financial stability.
Understanding CPT 92250
What Is CPT 92250?
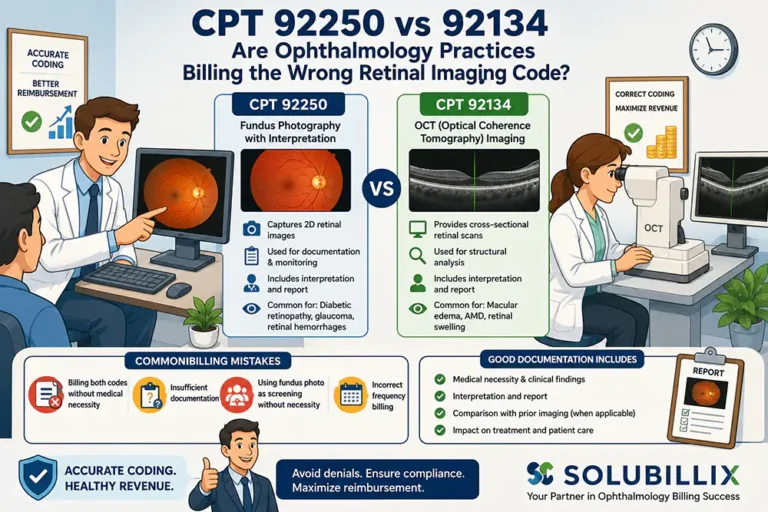
CPT 92250 is used for:
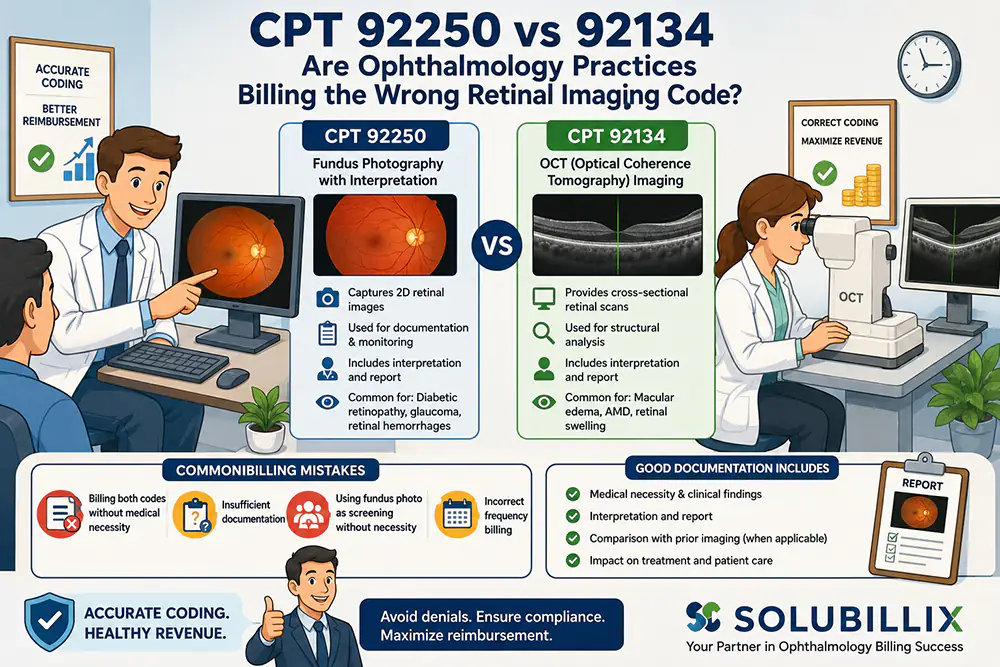
Fundus photography with interpretation and report
This procedure captures detailed photographic images of the retina, optic nerve, macula, and posterior segment of the eye. Fundus photography is commonly used to document and monitor:
- Diabetic retinopathy
- Glaucoma
- Retinal hemorrhages
- Hypertensive retinopathy
- Macular degeneration
- Optic nerve abnormalities
The code includes both the imaging procedure and physician interpretation.
Understanding CPT 92134
What Is CPT 92134?
CPT 92134 is used for:
Scanning computerized ophthalmic diagnostic imaging (SCODI) of the retina
This code primarily refers to Optical Coherence Tomography (OCT) imaging of the retina.
OCT technology provides cross-sectional retinal images that help physicians evaluate retinal layers and diagnose conditions such as:
- Macular edema
- Retinal swelling
- Vitreomacular traction
- Age-related macular degeneration
- Diabetic macular edema
Unlike fundus photography, OCT imaging provides structural retinal analysis rather than surface photographic documentation.
Why Ophthalmology Practices Confuse CPT 92250 and 92134
Many eye care clinics mistakenly believe these codes are interchangeable because both involve retinal imaging. However, insurance payers treat them as separate diagnostic procedures with different clinical purposes.
The confusion often occurs when practices perform both services during the same patient visit without understanding payer guidelines or documentation requirements.
This can lead to:
- Claim denials
- Duplicate service rejections
- Medical necessity audits
- Reduced reimbursement
- Compliance concerns
Key Differences Between CPT 92250 and CPT 92134
| Feature | CPT 92250 | CPT 92134 |
| Procedure Type | Fundus Photography | Retinal OCT Imaging |
| Imaging Method | Retinal photographs | Cross-sectional retinal scan |
| Primary Purpose | Documentation and monitoring | Structural retinal analysis |
| Technology Used | Fundus camera | Optical Coherence Tomography |
| Common Conditions | Diabetic retinopathy, glaucoma | Macular edema, retinal disease |
| Includes Interpretation | Yes | Yes |
Understanding these distinctions helps providers avoid incorrect code selection and payer disputes.
Common Billing Mistakes With CPT 92250 and 92134
1. Billing Both Codes Without Medical Necessity
One of the biggest mistakes occurs when providers bill both CPT codes during the same encounter without sufficient clinical justification.
Many insurance carriers consider these services overlapping unless documentation clearly supports separate medical necessity.
Without proper justification, claims may be denied or downcoded.
2. Insufficient Documentation
Payers require detailed clinical documentation to support retinal imaging claims.
Missing documentation may include:
- Physician interpretation
- Clinical findings
- Diagnostic rationale
- Treatment impact
- Comparison with prior imaging
Incomplete records are a major cause of ophthalmology claim denials.
3. Using Fundus Photography as a Screening Tool
Routine screening images without documented medical necessity are frequently denied.
CPT 92250 should only be billed when medically necessary for diagnosis or disease management.
4. Incorrect Frequency Billing
Some ophthalmology practices unknowingly exceed payer frequency limitations for retinal imaging.
Many insurance carriers restrict how often CPT 92134 or 92250 can be billed within a certain timeframe unless medical necessity is clearly documented.
5. Missing Interpretation and Report Requirements
Both CPT codes require a physician interpretation and formal report.
Simply storing retinal images in the patient chart is not enough to support reimbursement.
The interpretation should clearly explain:
- Clinical findings
- Diagnostic significance
- Disease progression
- Impact on treatment planning
Documentation Requirements for Accurate Reimbursement
To improve reimbursement success, ophthalmology practices should ensure documentation includes:
For CPT 92250
- Reason for fundus photography
- Retinal findings
- Physician interpretation
- Disease monitoring details
- Comparison to prior images when applicable
For CPT 92134
- OCT findings
- Retinal layer analysis
- Diagnostic significance
- Clinical assessment
- Treatment considerations
Strong documentation helps reduce denials and supports audit protection.
CMS and Payer Compliance Considerations
CMS and commercial insurance carriers closely monitor ophthalmology imaging utilization patterns.
Key compliance areas include:
- Medical necessity validation
- Frequency limitations
- Proper interpretation reports
- Avoiding duplicate billing
- Appropriate ICD-10 diagnosis linkage
Incorrect retinal imaging billing can trigger payer audits and reimbursement recoupments.
Because policies vary by payer, ophthalmology practices should regularly review carrier-specific billing guidelines.
How Solubillix Helps Ophthalmology Practices Reduce Billing Errors
At Solubillix, we specialize in ophthalmology and optometry revenue cycle management. Our billing experts help eye care practices improve coding accuracy, reduce denials, and optimize retinal imaging reimbursement.
Our ophthalmology billing solutions include:
- CPT coding audits
- Denial management
- Documentation review
- Retina imaging compliance support
- Insurance verification
- Revenue cycle optimization
- Specialty-focused billing workflows
By identifying coding gaps early, practices can prevent revenue leakage and strengthen long-term financial performance.
Frequently Asked Questions
Can CPT 92250 and 92134 be billed together?
Yes, but only when medically necessary and properly documented. Payers may deny claims if services appear duplicative.
Does CPT 92134 include physician interpretation?
Yes. CPT 92134 requires physician interpretation and report documentation for reimbursement.
Why are retinal imaging claims commonly denied?
Most denials occur because of missing medical necessity, incomplete documentation, frequency limitations, or incorrect code selection.
Final Thoughts
CPT 92250 and CPT 92134 are both essential ophthalmology diagnostic imaging codes, but they serve very different clinical purposes. Confusing these retinal imaging procedures can lead to claim denials, compliance risks, and lost revenue.
Ophthalmology practices that prioritize documentation accuracy, coding education, and payer compliance are better positioned to improve reimbursement outcomes and reduce audit exposure.
At Solubillix, we help ophthalmology and optometry practices simplify complex billing challenges through specialty-focused medical billing solutions designed to maximize revenue and strengthen operational efficiency.