1. Overview
Provider notes—also known as clinical documentation—are detailed records that capture everything a clinician observes, decides, and performs during patient care.
These notes are the foundation of accurate medical billing, as they prove that services were rendered, justify medical necessity, and protect providers in audits or disputes.
Without proper documentation, even legitimate medical services can be denied or underpaid by insurance carriers.
2. Main Types of Provider Notes and Their Billing Relevance
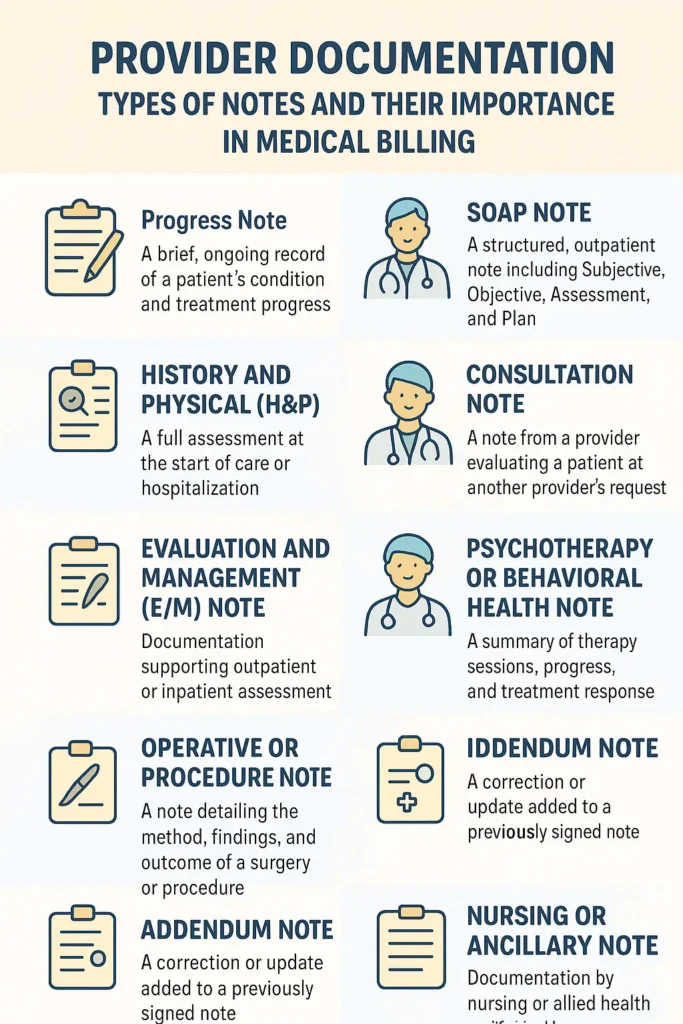
a. Progress Note
- Meaning: A brief, ongoing record showing how the patient’s condition evolves during treatment.
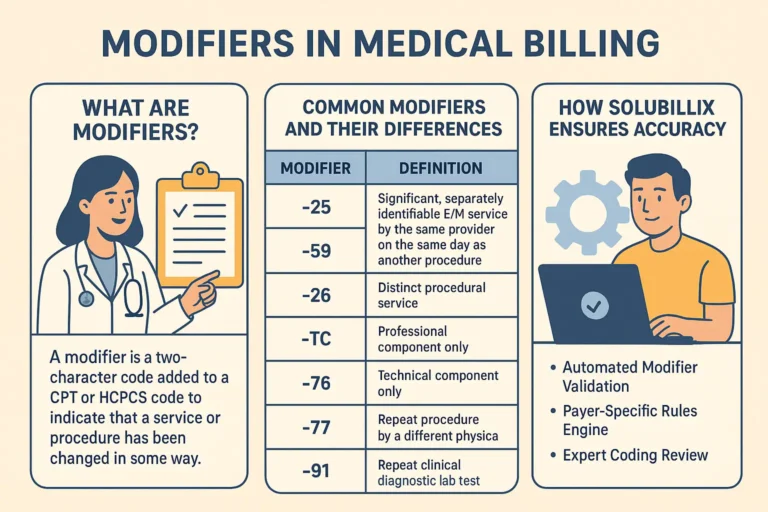
- Billing Relevance: Supports follow-up visits and ongoing care codes (e.g., CPT 99213–99214). Demonstrates medical necessity and continuity of care.
b. SOAP Note
- Meaning: A structured format commonly used in outpatient visits, broken into Subjective, Objective, Assessment, and Plan.
- Billing Relevance: Each element helps coders determine visit complexity and E/M level. SOAP notes clearly show the thought process that supports the level of service billed.
c. Comprehensive Note
- Meaning: A complete, detailed documentation including history, physical examination, and medical decision-making.
- Billing Relevance: Required for new patient visits and high-level encounters (e.g., 99204, 99205). Missing components can cause downcoding.
d. History and Physical (H&P)
- Meaning: A full assessment at the start of care or hospitalization outlining patient history, symptoms, and physical findings.
- Billing Relevance: Establishes the baseline of medical necessity for the admission or treatment plan.
e. Evaluation and Management (E/M) Note
- Meaning: Documentation supporting outpatient or inpatient assessment and management services.
- Billing Relevance: Determines the E/M level billed. Every payer review uses this note to verify if the level chosen matches the documented complexity.
f. Consultation Note
- Meaning: Created when a provider assesses a patient at another clinician’s request.
- Billing Relevance: Must include referring provider’s name, reason for referral, and findings. Missing this can result in denial of consult codes.
g. Operative or Procedure Note
- Meaning: Detailed record written immediately after a surgery or procedure describing methods, findings, and outcomes.
- Billing Relevance: Essential to justify procedural CPT codes. Auditors compare these notes directly with billed services.
h. Psychotherapy or Behavioral Health Note
- Meaning: Summarizes therapy session content, patient progress, and clinical response.
- Billing Relevance: Supports time-based psychotherapy codes (e.g., 90834, 90837). Start and end times are mandatory for insurance acceptance.
i. Discharge Summary
- Meaning: A final summary when the patient is released from inpatient care, detailing treatment course and follow-up instructions.
- Billing Relevance: Supports inpatient claims and transitional care management billing.
j. Addendum Note
- Meaning: A correction or clarification added after a note has been signed, explaining new or updated information.
- Billing Relevance: Shows transparency and compliance with audit standards.
k. Incident-to or Supervisory Note
- Meaning: Used when non-physician practitioners perform services under physician supervision.
- Billing Relevance: Required to meet incident-to billing guidelines under Medicare and certain commercial payers.
l. Nursing or Ancillary Note
- Meaning: Documentation by nursing or allied health staff detailing observations, vitals, or interventions.
- Billing Relevance: Supports facility-based charges and overall medical necessity.
3. Why Provider Notes Are Critical in Medical Billing
- Establish Medical Necessity
Notes prove that each service was reasonable and necessary for the patient’s diagnosis. - Support Accurate Coding
Coders depend on detailed documentation to assign correct ICD-10, CPT, and HCPCS codes. - Ensure Compliance and Audit Protection
Proper documentation meets payer, HIPAA, and CMS compliance standards, reducing audit risks. - Facilitate Continuity of Care
Each provider involved can follow the patient’s progress, improving safety and outcomes. - Legal and Risk Protection
In disputes or legal reviews, provider notes serve as the official, time-stamped record of care.
4. Common Documentation Errors That Delay Payment
- Missing provider signature, date, or credentials
- Incomplete or template-based cloned notes
- Lack of session start and end times (for behavioral health)
- Failing to link diagnoses to CPT codes
- Using unclear abbreviations or handwriting
5. How Billing Partners Like Solubillix Help Ensure Compliance
A qualified billing partner ensures accuracy and compliance through:
- Pre-submission audits to detect missing credentials or signatures.
- E/M level validation based on documentation.
- Real-time feedback to providers for incomplete or missing notes.
- Ongoing training to maintain payer-specific compliance standards.
By integrating documentation review into the billing workflow, both denial rates and payment delays are significantly reduced.
✅ Conclusion
Provider documentation is not just a record—it’s the proof of care, compliance, and professionalism. Each note type plays a vital role in ensuring that every patient encounter is accurately represented, appropriately coded, and fully reimbursed.
Strong, clear, and compliant documentation builds the bridge between quality care and financial integrity.